
Ringing in the New Year
January 11, 2021
The Dystonia Coalition
September 16, 2021Dr. Aparna Wagle-Shukla
Dystonia is the third most common type of movement disorder. Dystonia occurs due to abnormal firing of brain signals that cause excessive and involuntary or out-of-control muscle contractions. As a result, patients develop abnormal twisting postures, involuntary movements, and lose motor control. Dystonia can affect muscles in either a single or multiple body regions. Examples of such regions include eyelids, face, jaws, neck, vocal cords, torso, limbs, hands, feet, or the entire body. For example, in some individuals with a genetic mutation in a gene called ‘DYT-TOR1A,’ the whole body is commonly affected, and such dystonia is referred to as generalized Dystonia.
How is dystonia managed?
Focal symptoms in a single body region are usually controlled with oral medications and/or botulinum toxin injection treatments. However, when dystonia is generalized, a significant majority of patients require additional surgical treatments. Many times, dystonia is accompanied by other motor symptoms such as tremor, parkinsonism, and myoclonus. Recently, dystonia has been found to affect patients’ mood, sleep, cognition, and balance, referred to as nonmotor symptoms. Therefore, many patients require multidisciplinary care to treat the numerous aspects of dystonia symptomatology successfully.
What oral medications are available for treating dystonia?
Oral medications for dystonia control the abnormal firing of brain signals. These medications modulate the functions of brain chemicals such as acetylcholine, gamma-aminobutyric acid, or GABA, glutamate, and dopamine that are usually involved in the signaling process.
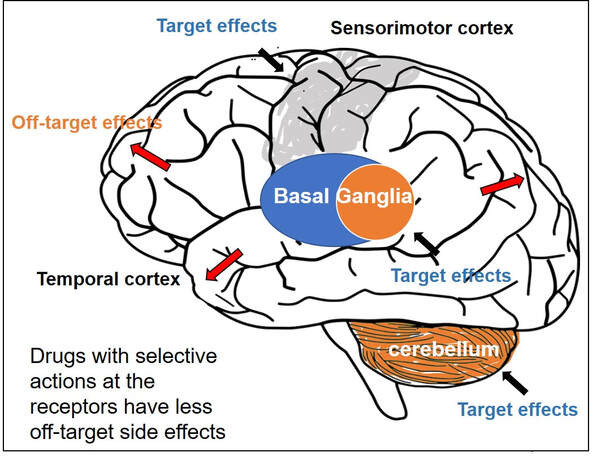
Animal models have shown acetylcholine signaling involving muscarinic receptors in the basal ganglia neurons is abnormal in dystonia. These neurons are located at the base of the brain. In a knock-in mouse model, drugs blocking these receptors (anticholinergic) were observed to reduce dystonia. Medications blocking acetylcholine effects at the muscarinic receptors have been among the oldest treatments available in clinical practice. Trihexyphenidyl (Artane) and benztropine (Cogentin) are commonly prescribed anticholinergic medications and have been observed to effectively treat dystonia symptoms. However, these two drugs non-selectively block all types of muscarinic receptors in the brain (M1, M2, M3, M4, and M5). Thus, side effects related to off-target stimulation such as confusional behavior and constipation are major limiting factors. Scientists have found that selectively blocking M4 receptors, which are highly concentrated in the basal ganglia neurons, will likely result in better clinical outcomes. These selective drugs, with potentially greater benefits and fewer side effects, are currently in the development phase. They will need to be tested and proven to be beneficial in clinical trials before they can be prescribed in clinical practice
Drugs targeting GABAergic receptors, including benzodiazepines (clonazepam, diazepam, and lorazepam) and baclofen, are other commonly used agents for treating dystonia. GABA is an inhibitory neurotransmitter. An increase in GABA signaling leads to the alleviation of excessive muscle contractions. A recent survey involving more than 2000 dystonia patients found benzodiazepines were the most common oral drugs prescribed for individuals with generalized dystonia, whereas botulinum toxin injections (another powerful muscle relaxant) were most frequently employed for treating focal dystonia. Zolpidem is a medication that also modulates GABA receptors in a slightly different way. It was used in a small study of 34 patients with focal dystonia. The study found significant improvements, but further research is needed on whether the clinical benefits can be extended to generalized dystonia, such as the DYT-TOR1A dystonia. Dopamine and dystonia have a complex relationship as medications that increase dopamine or decrease dopamine can improve clinical symptoms in certain forms of dystonia. Drugs such as levodopa-carbidopa, pramipexole, and ropinirole increase dopamine signaling, and drugs like tetrabenazine and deutetrabenazine decrease dopamine signaling through dopamine depletion.
Drug development can be an extremely lengthy and costly process. Thus, many clinical trials repurpose drugs to leverage their pharmacological properties for benefiting a broader range of clinical applications. One example is escitalopram (Lexapro), a selective serotonin reuptake inhibitor, a drug frequently used to treat pain and depression and generally well tolerated was recently found to improve cervical dystonia symptoms. The benefits were observed to be independent of their influence on mood circuitry. Another example is Perampanel, a drug antagonizing the action of glutamate neurotransmitter and approved for the treatment of epilepsy. Perampanel was recently tested in focal dystonia as the target receptors are widely distributed in the basal ganglia neurons. The target receptors are also seen in other neurons like the cerebellar neurons important for dystonia. While the drug was safe and tolerated by most patients, further studies are needed to confirm clinical efficacy.
What are the general principles for using oral medications?
Oral medications should be initiated at low doses and titrated up slowly to avoid off-target side effects, especially in older patients. Sometimes for certain medications like anticholinergic drugs, peak benefits are observed only weeks after maintaining constant doses. If the peak benefits are not adequate or are short-lasting, a further buildup of doses is recommended. If dose-limiting side effects develop with further escalation, an additional line of therapy is needed to achieve the best possible symptom control.
Are treatments available if a specific cause or etiology is identified?
In some individuals with dystonia, a specific cause can be identified. For example, when dystonia occurs due to a deficiency of enzymes needed to synthesize dopamine, the replacement of dopamine is found to alleviate symptoms (dopa-responsive dystonia). Sometimes dystonia is related to abnormalities in protein or lipid metabolism or deposition of heavy metals in the brain (e.g., copper, iron). In these circumstances, once the diagnosis is confirmed, appropriate specific therapies can be initiated.
References
Update on current and emerging therapies for dystonia; Karlo J Lizarraga, Duha Al-Shorafat & Susan Fox. Neurodegener. Dis.Manag. (2019) 9(3), 135–147
Anticholinergic drugs rescue synaptic plasticity in DYT1 dystonia: role of M1 muscarinic receptors. Maltese M, Martella G, Madeo G et al Mov. Disord. 29(13), 1655–1665 (2014
Dystonia treatment: patterns of medication use in an international cohort. Pirio Richardson S, Wegele AR, Skipper B, Deligtisch A, Jinnah HA. Neurology 88(6), 543–550 (2017).
Discovery of the first selective M4 muscarinic acetylcholine receptor antagonists with in vivo anti-parkinsonian and anti-dystonic efficacy. Mark S. Moehle, Aaron M. Bender, Jonathan W. Dickerson, et al. doi:
https://doi.org/10.1101/2020.10.12.324152


{kind=link}
{kind=link}
{kind=link}